Light Therapy Insights, Delivered
Get practical guidance, new device reviews, and research summaries written for real people.
You’re in. Watch your inbox soon.
Oops! Something went wrong while submitting the form.
Light Therapy Insights
Get practical guidance, new device reviews, and research summaries written for real people.
Can red light therapy relieve joint pain? Clinical research on photobiomodulation for osteoarthritis, rheumatoid arthritis, and chronic inflammation. Wavelengths, protocols, and realistic outcomes.
Joint pain affects over 90 million adults in the U.S. alone, and the limitations of conventional treatments — NSAIDs with gastrointestinal risks, opioids with addiction potential, and joint replacements with long recovery times — have driven significant interest in non-invasive alternatives. Red light therapy, particularly using near-infrared (NIR) wavelengths, has accumulated a compelling body of evidence for joint pain and inflammation. (For foundational context, see our evidence-based light therapy overview.)
Joint pain relief through photobiomodulation operates through mechanisms distinct from surface-level skin treatments:
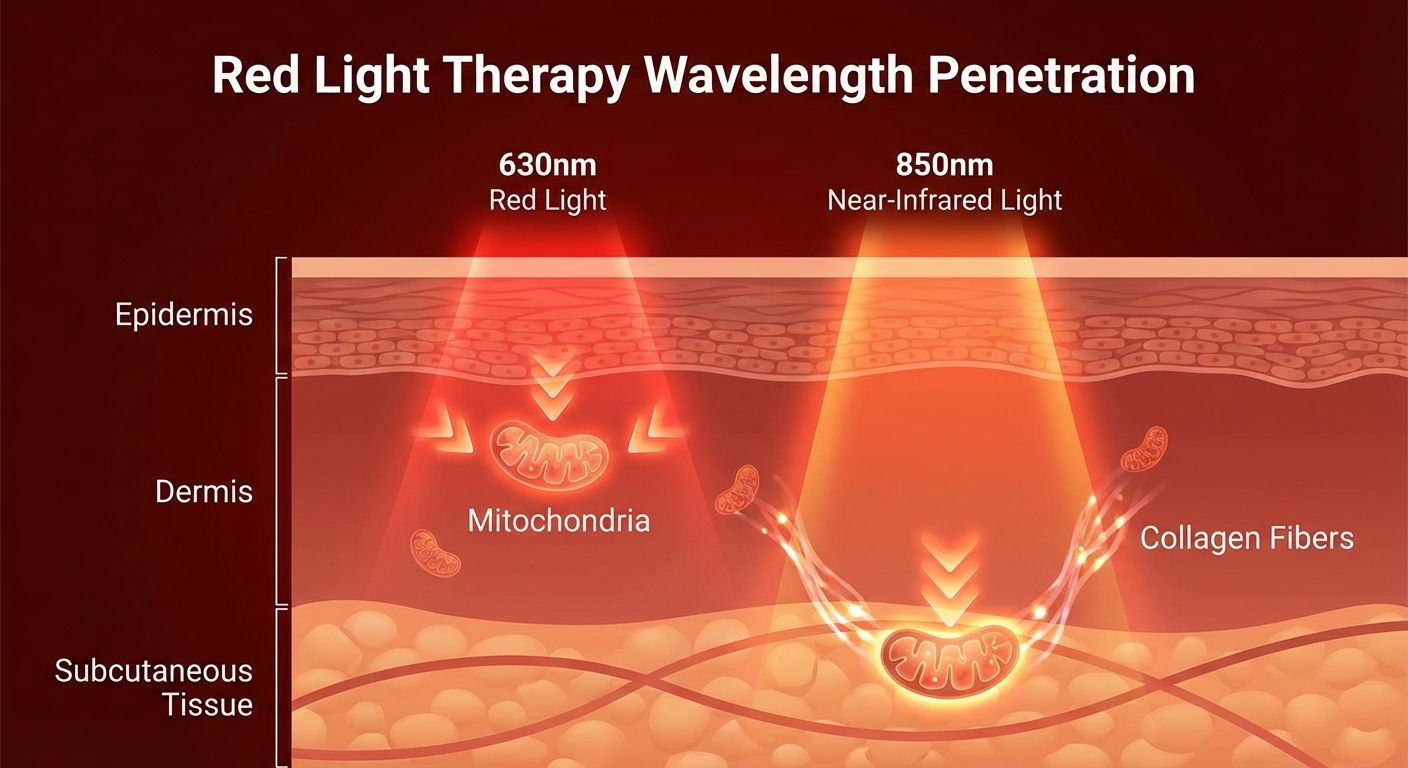
Deep Anti-Inflammatory Action: Near-infrared wavelengths (810–850nm) penetrate 5–30mm+ into tissue, reaching the synovial membrane, cartilage, and surrounding joint structures. At this depth, NIR light reduces pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) while upregulating anti-inflammatory mediators. Unlike NSAIDs that mask inflammation, photobiomodulation appears to modulate the inflammatory cascade at its source.
Pain Signal Modulation: Research shows that NIR light affects nerve conduction velocity and nociceptor sensitivity, effectively raising the pain threshold. Some studies demonstrate direct analgesic effects independent of anti-inflammatory action.
Cartilage Protection: Emerging research suggests photobiomodulation may support chondrocyte (cartilage cell) metabolism and slow cartilage degradation. This is particularly relevant for osteoarthritis, where progressive cartilage loss is the primary pathology.
Improved Circulation: NIR light stimulates nitric oxide release and angiogenesis around joints, improving nutrient delivery and waste removal from joint tissue. For a detailed explanation of how NIR differs from visible red light, see our NIR vs. red light guide.
Osteoarthritis (OA) has the strongest evidence base for red light therapy among joint conditions. A 2009 Cochrane systematic review examined multiple RCTs and found that LLLT reduced pain by up to 70% and improved function in knee osteoarthritis patients. A 2019 meta-analysis in Clinical Rehabilitation confirmed these findings, showing statistically significant reductions in pain and stiffness, improved joint mobility and function, and decreased morning stiffness duration. The most effective protocols used 810–850nm wavelengths, applied directly over the affected joint for 10–20 minutes per session.
Research on RA is more limited but promising. Small RCTs have shown reduced hand stiffness and pain, improved grip strength, and decreased morning stiffness duration. The anti-inflammatory mechanism is particularly relevant for RA, an autoimmune condition driven by chronic inflammation.
Multiple studies support NIR therapy for Achilles tendinopathy, lateral epicondylitis (tennis elbow), rotator cuff injuries, and plantar fasciitis. The combination of anti-inflammatory and tissue-healing effects makes photobiomodulation a strong adjunct to physical therapy for these conditions.
Joint tissue is deeper than skin, making wavelength selection critical:
810–850nm (Near-Infrared): The primary wavelength range for joint conditions. These wavelengths penetrate deep enough to reach most joints. This is where the majority of positive joint-related research has been conducted. 660nm (Red): Useful for superficial joint structures and complementary anti-inflammatory effects, but doesn't penetrate deep enough on its own for significant joint benefit. Combination approach: Devices offering both 660nm and 850nm provide surface-level inflammation reduction plus deep joint penetration.
Device positioning: Direct contact or within 1–2 inches of the affected joint for maximum penetration. For panels, position the joint 6–12 inches from the device surface.
Duration: 10–20 minutes per joint per session. Larger joints (knee, hip) may benefit from treating from multiple angles — front and back of the knee, for example.
Frequency: Daily treatment during acute pain phases. 3–5 times per week for chronic conditions. See our frequency guide for general protocol principles.
Timeline: Some users report pain relief within the first few sessions (analgesic effect). Anti-inflammatory benefits typically become apparent within 2–4 weeks. Functional improvements (mobility, stiffness reduction) often take 4–8 weeks. Maximum benefit is usually reached at 8–12 weeks of consistent use.
For joint-specific treatment, you need a device with adequate NIR output:
Full-Body Panels: The most versatile option. Treats joints, skin, and muscle simultaneously. See our panel buyer's guide.
Compact Panels or Pads: More affordable and targeted. Good for single-joint treatment (knee, elbow, shoulder). Wrap-style LED pads can conform to joint contours for better coverage.
LED Face Masks: Not appropriate for joint treatment — wrong form factor and typically lack adequate NIR power for deep tissue penetration.
For detailed guidance on evaluating device specifications, see our complete buyer's guide.
Physical Therapy: Red light therapy before exercise or PT sessions can reduce pain and improve range of motion, allowing more effective rehabilitation.
Topical Anti-Inflammatories: Apply after light therapy sessions for potentially enhanced absorption through increased tissue circulation.
Joint Supplements: Glucosamine, chondroitin, and collagen peptides support cartilage health from a nutritional angle while light therapy works at the cellular level.
Exercise: Regular, joint-appropriate exercise is essential for managing arthritis. Light therapy can help manage the pain that often limits exercise participation.
Red light therapy is well-tolerated for joint applications. However, it is not a cure for progressive joint disease, should not replace medical evaluation for new or worsening joint symptoms, and may not be sufficient as a standalone treatment for severe osteoarthritis or advanced RA. For complete safety information including contraindications, see our safety guide.
Red light therapy — particularly near-infrared wavelengths — offers a well-researched, non-invasive option for managing joint pain and inflammation. The evidence is strongest for knee osteoarthritis, with promising results across other joint conditions. Combined with appropriate medical care, exercise, and consistent use over 4–12 weeks, photobiomodulation can be a valuable addition to a joint health strategy.
Get practical guidance, new device reviews, and research summaries written for real people.





